IJERPH | Free Full-Text | Artificial Intelligence as a Decision-Making Tool in Forensic Dentistry: A Pilot Study with I3M
Feature papers represent the most advanced research with significant potential for high impact in the field. A Feature
Paper should be a substantial original Article that involves several techniques or approaches, provides an outlook for
future research directions and describes possible research applications.
Feature papers are submitted upon individual invitation or recommendation by the scientific editors and must receive
positive feedback from the reviewers.
Editor’s Choice articles are based on recommendations by the scientific editors of MDPI journals from around the world.
Editors select a small number of articles recently published in the journal that they believe will be particularly
interesting to readers, or important in the respective research area. The aim is to provide a snapshot of some of the
most exciting work published in the various research areas of the journal.
Artificial Intelligence as a Decision-Making Tool in Forensic Dentistry: A Pilot Study with I3M
Int. J. Environ. Res. Public Health 2023, 20(5), 4620; https://doi.org/10.3390/ijerph20054620 (registering DOI)
Decision-making is a daily process used in all medical fields including dentistry. In forensic medicine, age estimation has become an important challenge as biological markers vary notably from person to person, even in the context of identical chronological age [
1]. Therefore, this context constitutes a good pilot study for the development of a decision-making procedure aiming at categorizing one individual’s age. More specifically, one of the most challenging issues involving living patients is to assess whether a person is a minor or not (i.e., under or over 18 years of age) [
2]. This question is especially key in the context of unaccompanied asylum seekers without reliable documentation. The protocol of the Study Group on Forensic Age Diagnostics (AGFAD) for age estimation recommends combining a clinical examination (including the oral cavity), a hand radiograph, an orthopantomogram (OPG), and a CT scan of the clavicle medial end (if the skeletal development of the hand and wrist is completed) [
3]. Following this recommendation, several techniques based on OPGs have been proposed to estimate the age of a given individual [
4,
5]; however, there is currently no scientific consensus regarding the best strategy.
Nearly fifteen years ago, Cameriere et al. [
6] developed a topological method to estimate whether the chronological age of a given person is below or above 18 years. This approach is based on the relationship between the age and the third molar maturity index (I3M), which takes into account the apex width (a and b, respectively, for the mesial and distal apex width) and the tooth height (c) by computing the ratio: (a + b)/c [
6,
7]. A threshold (cut-off) value of I3M < 0.08 was identified and used to discriminate between minors and adults. This method has later been applied to several populations and has been shown to be the most efficient in discriminating between these two categories [
8,
9,
10].
Thus, the aim of the present pilot study was to investigate the technical feasibility of creating a decision-making tool based on the I3M index for forensic experts. This study presented an automated approach consisting of a mask inference on OPG followed by a topological analysis with or without a deep learning component. Performance was computed for each task, and the accuracy of their combination was finally investigated in comparison with the forensic expert’s I3M estimation. The null hypothesis was, therefore, that the I3M inferred by the solution is identical to the one estimated by the expert.
This study was conducted with accordance of the local ethical committee (HCL-21_440). A retrospective set of 530 OPGs was obtained from a previous French study [
8] and thanks to an international collaboration with the Hospital of Mulago (Uganda; ethical validation SBS-216). The image collection was performed in accordance with local and national ethical standards and the Declaration of Helsinki and its later amendments. The present study was conducted and reported following as much as possible the recommendations on artificial intelligence in dentistry [
24], more specifically, on the 25 items presented in the article, 23 were followed while two others (clustering and missing data management) were not applicable in our context. The OPGs were first cropped to extract left and right mandibular third molar images downsized to 256 × 256 pixels, a reasonable resolution for experts to distinguish the dental details and therefore properly assess the I3M score. Each image was analyzed by an I3M expert (CT) to assess the possibility of estimating an I3M score. Among others, radiographs without two apices or without a third mandibular molar were excluded. The final reviewed dataset was composed of 456 images, 57% of the patients were minor for an average age of 17.9 years.
A model is defined as the combination between a segmentation algorithm (mask R-CNN [
25] or U-Net [
26]) with one computing the I3M through a topological analysis with or without a deep learning component. In order to assess the performance of each model, 80% of the database was assigned to the training sample, and the remaining 20% to the testing sample, which was solely used to compute the statistical error once the model was trained. Before training and testing Mask R-CNN [
25] and U-Net [
26] (see below), a data pre-processing procedure was applied using the contrast limited adaptive histogram equalization (CLAHE) enhancement approach. This image processing enhances the contrast through a transformation function based on the neighborhood region of each pixel [
27]. Data augmentation techniques were also applied using random rotations and flips of the images.
Two deep learning approaches were used and compared to perform the mask inference: Mask R-CNN and U-Net.
Mask R-CNN is a region-based convolutional neural network, its backbone is the Faster-RCNN algorithm with an additional final convolutional branch enabling the prediction of an object mask [
25]. Mask R-CNN is an algorithm developed by the Facebook AI Research team and was implemented, in our context, under the open MIT License (matterport) [
29]. U-Net is a convolutional neural network with a characteristic U-shaped architecture that was specifically developed for biomedical image analysis and has already proven to be successful in analyzing tooth decay on X-ray images [
26].
2.5. Topological Data Analysis without Deep Learning (TDA) or with Deep Learning (TDA-DL)
Topological Data Analysis (TDA) consists in the application of the mathematic discipline of topology to data extracted from a real system allowing the analysis of geometrical patterns such as shapes [
30]. Two specific approaches were compared to compute the I3M figures based on a segmented tooth (mask).
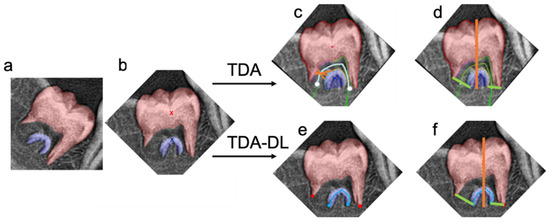
The first step of TDA consisted of the rotation of the image by vertically aligning the barycenters of the two instances segmentations in order to compute the tooth height (parameter c). The second step consisted of applying a gradient approach to find the line equidistant to both instance segmentations. This line represented the root canal center, its ending points were the middle of the apices. The final steps consisted of finding the two extremities of each apex. Simulation of radii centered on various points of the centered line were used to partition each instance segmentation in two parts: one separating the pulp and the dentine, the other separating the tooth and the environment. The extremity of the apex constituted the transition between these two parts. Finally, the a, b, and c parameters were computed: a and b corresponded to the distance between the two extremities of each apex, and c was the distance between the lowest and the highest point on the vertical axis.
The TDA-DL approach consisted in combining a topological data analysis followed by a deep learning approach. The first step was the rotation of the image by vertically aligning the barycenters of the two instances segmentations (apical and coronal) in order to compute the height (parameter c) of the tooth. The segmentations (apical and coronal) were then virtually separated into two sections by a vertical line joining the barycenters. The coronal limit points were defined, on the left and right side of the vertical line, as the lowest points of the coronal segmentation. In order to find the apical limit points, a deep learning approach was implemented. It consisted in fitting an inverted U-shape line at the center of the apical mask. The U-shape line was mathematically defined by five points: two ending points and three inflexion points. A U-Net convolutional network was trained to infer this apical mask skeleton. The apical limit points were then defined, on the left and right side of the vertical line, as the ending points of the inferred U-shape skeleton. The a and b parameters were then computed as the distance between the coronal and apical ending points on the left side and on the right side, respectively, of the vertical middle line (
Figure 1).
In order to properly assess the error related solely to the topological analysis, the algorithm was also applied on ground truth segmentations. The inferred metrics, a, b, and c were then compared to the expert’s ones.
In order to assess the impact of the error on the final decision, the I3M threshold was set to 0.08: for I3M < 0.08, the subject was considered as being ≥18 years old, for I3M > 0.08, the subject was considered as being <18 years old.
In order to analyze the ability of the automated approach to compute I3M, a paired bilateral T-test analysis was performed with a type 1 error of 0.01.
This approach was used to compare the I3M inferred by the complete automated solution combining the deep learning and the topological approach to the expert’s one. It was also used to compare the I3M inferred by the topological analysis on the ground truth mask to the expert’s one to isolate the error inherent to the second part of the process.
Analysis of the performance of the different algorithms regarding the final decision was performed using the McNemar’s test for nominal data and the null hypothesis was the presence of an agreement.
Pearson correlations were also computed to estimate the linear dependency between the expert’s I3M and the one computed by the various algorithms.
Paired sample
T-test of bilateral difference demonstrated a significative difference between Mask R-CNN and U-Net for the segmented masks, the apical masks, and the overall masks. In terms of mean intersection over union, U-Net performed better than Mask R-CNN for the coronal mask (U-Net: 92.9%; Mask R-CNN: 86.1%), the apical mask (U-Net: 74.8%; Mas R-CNN: 62.1%) as well as the overall mask (U-Net: 91.2%; Mask R-CNN: 83.8%) (
Table 1).
At this stage, in the training sample, approximately two thirds of the OPGs (57/88) were kept, which corresponded mostly to underage subjects (80% of the sample). Indeed, the remaining 31 OPGs presented closed or almost closed apices, which made it difficult for U-Net to identify the two different parts of the tooth, and therefore for TDA or TDA-DL to identify the two apices.
Topological analysis on the ground truth mask revealed similar performance between TDA and TDA-DL. TDA was able to determine a + b with a mean absolute error (MAE) ± standard deviation (SD) of 12.26 ± 7.21 pixels in comparison with the value of the expert, while the TDA-DL MAE ± SD was 17.98 ± 9.08 pixels (
Figure 3). Similarly, for c, the MAE ± SD was 26.67 ± 9.97 pixels for TDA and 26.21 ± 10.28 pixels for TDA-DL (
Figure 4). Paired
T-test analysis for TDA and TDA-DL on ground truth found
p-values < 0.01, thereby rejecting the null hypothesis of similarity between the expert and the various combinations.
The combined approach consisted in implementing the best segmentation algorithm followed by the different topological analyses in order to compare their ability to predict the I3M score. The MAE ± SD was 0.04 ± 0.03 for U-Net combined with TDA and 0.06 ± 0.04 for U-Net combined with TDA-DL in comparison with a dental forensic expert. Both these combinations were able to reproduce 94.7% (54/57) of the expert decisions.
Analysis of the final decision based on the I3M score revealed a non-rejection of the McNemar test for any of the combinations considered, suggesting that the expert and algorithm combinations mainly agreed on the final decision.
The aim of this study was to evaluate the feasibility of replicating the cognitive mechanism of a forensic expert using an innovative approach consisting in the combination of supervised deep learning approaches and automated topological algorithms. The results suggested that U-Net was the best approach to infer the mask of the mandibular third molar. They also revealed that the two topological approaches offered similar performance regarding their ability to properly infer a, b, and c, and therefore the I3M score. The developed approach was able to mimic the forensic expertise with a 94.7% accuracy. However, several methodological, technical, and ethical questions must be discussed.
Regarding the overall performance, U-Net combined with TDA or with TDA-DL displayed a 95% accuracy in comparison with the expert’s decision, which is promising for this first pilot study. It is important to note that these results were obtained on a database with an 80% share of underage patients given the necessity to have a large panel of open apices radiographs. Indeed, compared to other similar studies [
39,
40], the present study presented a relatively low number of OPGs, which might have limited the algorithm’s ability to learn all possible root configurations, and one could reasonably expect better results with a larger training database.
Graphical analysis between the expert’s measurements and the ones produced by the algorithm revealed a systematic overestimation by the latter. These discrepancies can be explained by the fact that the algorithm used the crown’s most coronal point when estimating the c value, while the expert used a reference point that is more centered on the crown; regarding a and b, the algorithm by design measured the distance between the two most apical points while the expert used points that are slightly more coronal, in other words the expert estimated a width at the apical constriction while the algorithm estimated it at the apical foramen.
This pilot study also highlighted several limitations that must be discussed. First and foremost, this study was performed on a relatively small database, even when considering the effect of data augmentation. Its results should therefore be considered with care, they are only reflecting the potential of such approach in the context of this pilot study which calls for further studies with similar approaches on a larger sample size in order to eventually consider the generalization of this solution. Moreover, the present study was performed after a manual cropping of the third molar, which limited its ease of use but also led to better results. A future perspective would be to implement an automated cropping of the mandibular third molars, such an approach appears to be relatively easy according to published studies [
21,
32]. It is also important to note that major differences could exist between populations, but also between OPGs themselves, thereby leading to different root configurations, positions, and radiograph qualities, potentially increasing the errors during the labeling and I3M computation [
41]. Previous studies based on unsupervised approaches have offered very few explicability tools and oftentimes display direct raw results without giving the user the possibility of evaluating the intermediary step leading de facto to black box models. Notwithstanding, it is worth mentioning the Grad-CAM heat map that was proposed to improve the explicability of deep-learning-supervised solutions [
4]. By reporting the masks and displaying the a, b, and c segments on the radiograph, the procedure proposed herein allows any expert or user to visually validate the mask inference as well as the computation of the score, thereby greatly improving the overall explicability and transparency. A selection bias is also inherent to the expert’s filtering process. As a matter of fact, the selection criterion was radiographic images compatible with the computation of an I3M score. In other words, only teeth with open apices were selected, leading to the creation of a subject sample for which the average age was lower than 18 years. However, further investigations could lead to the production of an algorithm able to identify the tooth stage or closed apex on a given radiograph, and therefore compensate for this bias [
21,
42]. Furthermore, this pilot study based itself on a single forensic expert and a relatively small database mixing radiographic images from two countries. In this context, the generalization of the proposed approach would require more extensive research on a larger, more diverse database, as well as the comparison to a panel of several I3M experts.
Finally, some ethical questions relative to the use of AI-based technologies could be raised [
43], especially given the legal impact that any mistakes could have. This question is challenging; however, with respect to EU law, most of the time, the responsibility is transferred to the user (i.e., the expert) [
44]. It therefore requires particular care when distributing such a technology. Critically, the aim of this study was to estimate the technical feasibility of developing a tool for educational purposes or to assist experts in uncertain cases, especially when the score averages around 0.08; this study never intended to replace forensic experts. This fully transparent approach offering visual results to the final user is particularly important since AI in dentistry is a fairly recent field of investigation, trust must be gained in order to obtain a sustained and fully accepted system [
43,
44,
45,
46].
This study was able to segment mandibular third molars in two parts and measure the apex width (a and b) as well as the tooth height (c). The best approach consisted in a U-Net algorithm combined with a topological approach. This study illustrated the technical feasibility of creating a decision-making tool replicating the I3M index for forensic experts with a 95% accuracy and a mean absolute error of 0.04. However, due to the numerous limitations highlighted by this proof-of-concept, further investigations are required before considering generalization and implementation of the solution.
Data are available by contacting the corresponding or first authors.
Figure 1.
Illustration of the Topological Data Analysis (TDA) and Topological Data Analysis associated with Deep Learning (TDA-DL). Both approaches (TDA and TDA-DL) take as an input the (a) instance segmentation, (b) vertical rotated based on the barycenters (red and blue x). The TDA approach finds the (c) root canal middle line (cyan) based on the gradient analysis between the apical and coronal segmentation. Then, the segmentation of the root canal walls is obtained through radii analysis (orange) centered on the root canal middle line (cyan). The last points of the coronal and apical root canal walls on the left and right side of the tooth represent the ending points necessary to compute the apex diameter. (d) A vertical line joining the barycenters is defined in order to measure of the tooth height, more specifically this line cannot go above the most coronal point of the instance segmentation nor below the most apical point of the instance segmentation. The TDA-DL approach directly applies a deep learning approach able to automatically find the (e) root canal ending points (blue, red) and then (f) measure the tooth height and apex diameter using the obtained points.
Figure 2.
Illustration on three different radiographs (a–c) of the segmentation and its associated error with Mask-R CNN (d–f) and U-Net (g–i). Green: true positive, orange: false positive, red: false negative, #: illustration of Mask R-CNN errors on the apices, *: illustration of Mask R-CNN error on the crown.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
Bui, R.; Iozzino, R.; Richert, R.; Roy, P.; Boussel, L.; Tafrount, C.; Ducret, M. Artificial Intelligence as a Decision-Making Tool in Forensic Dentistry: A Pilot Study with I3M. Int. J. Environ. Res. Public Health 2023, 20, 4620.
https://doi.org/10.3390/ijerph20054620
Bui, Romain, Régis Iozzino, Raphaël Richert, Pascal Roy, Loïc Boussel, Cheraz Tafrount, and Maxime Ducret. 2023. “Artificial Intelligence as a Decision-Making Tool in Forensic Dentistry: A Pilot Study with I3M” International Journal of Environmental Research and Public Health 20, no. 5: 4620.
https://doi.org/10.3390/ijerph20054620
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details
here.
This content was originally published here.